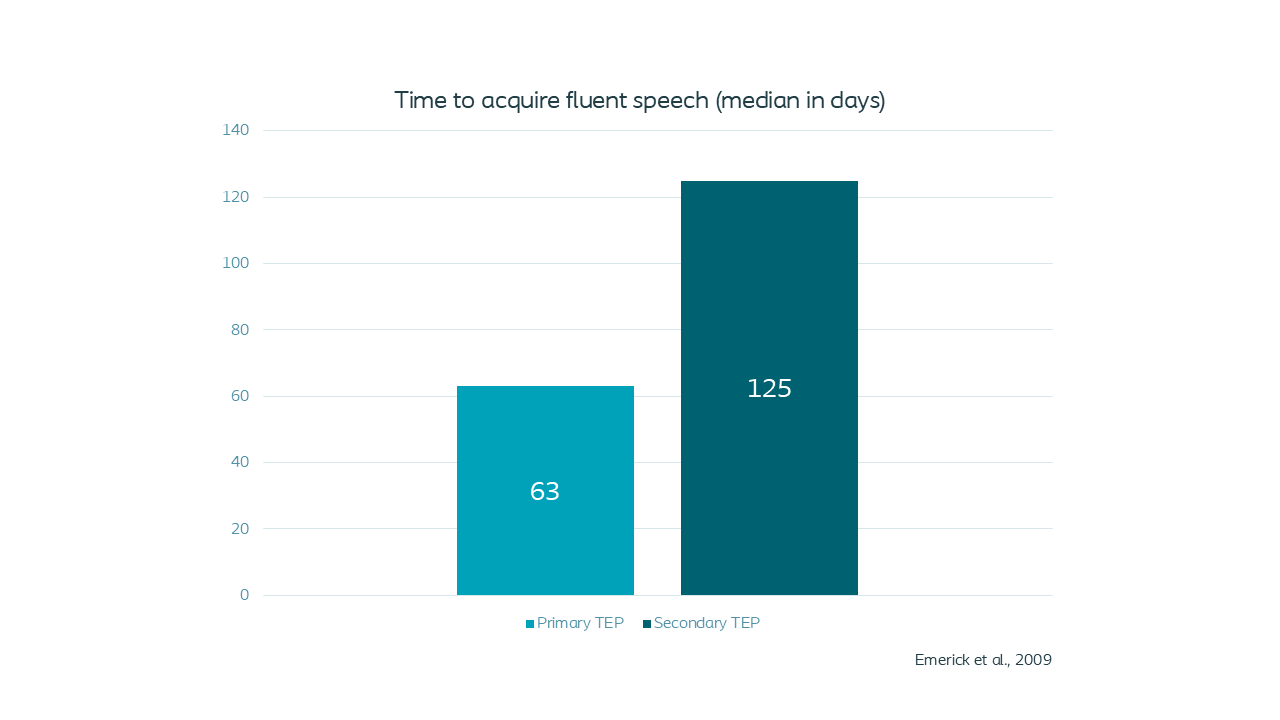
Primary punctures allow for earlier voice rehabilitation
Patients who underwent primary puncture achieved fluent speech 62 days earlier than patients who underwent secondary puncture(1).

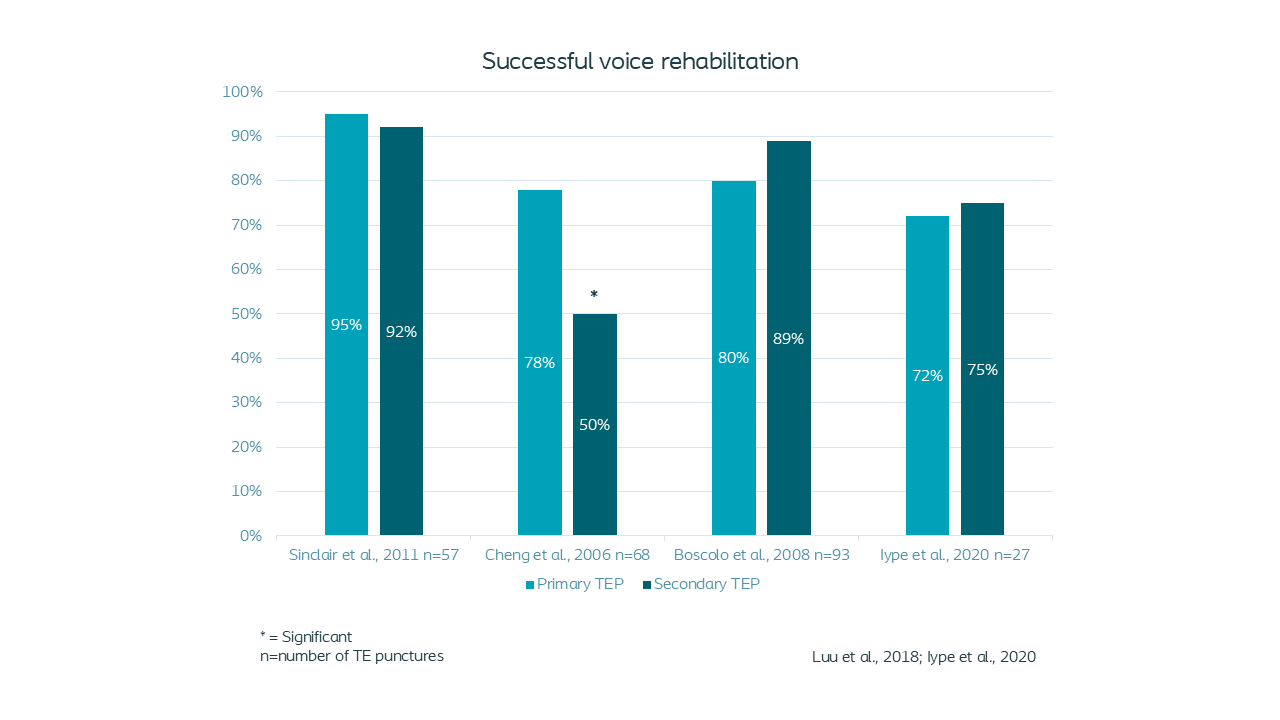
Primary punctures allow for successful voice rehabilitation
Clinical evidence shows overall success rates and voice outcomes were similar between primary and secondary TEP(2-6).

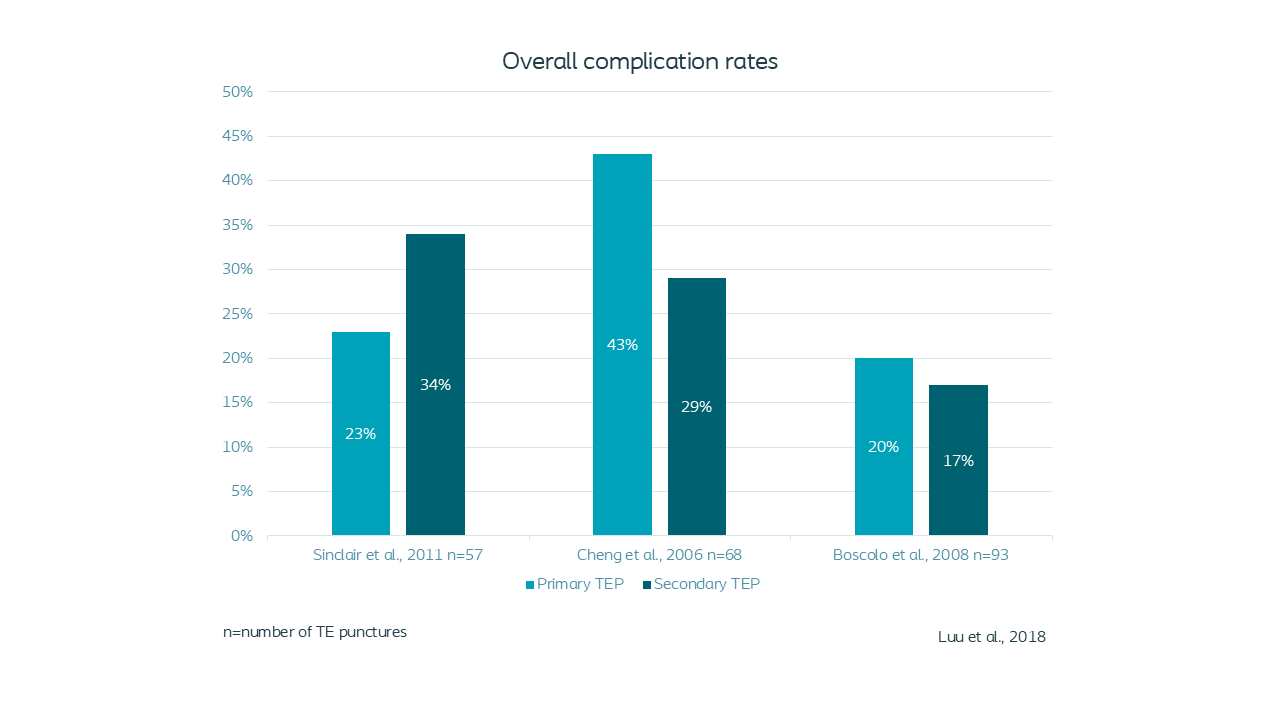
No difference in complication rates between primary and secondary punctures
Systematic review shows primary puncture is not associated with higher complication rates compared to secondary puncture. With primary placement no TEP catheter is needed, potentially minimizing tissue trauma(2-5).

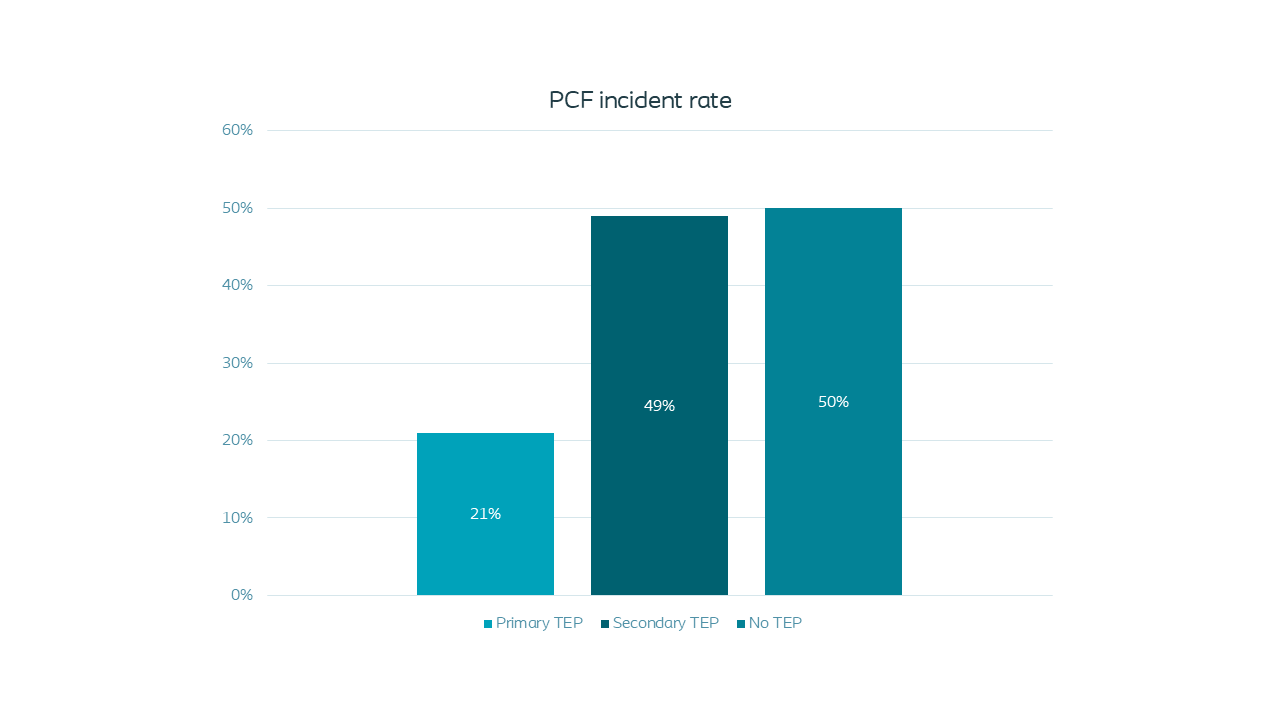
No increased risk of pharyngocutaneous fistula with primary punctures
Clinical evidence shows no increased risk of developing pharyngocutaneous fistula with primary puncture compared to secondary or no puncture(7).